

Coding and medical record documentation reminders for behavioral health claims
It’s no secret that mental health and substance abuse disorders have been on the rise in recent years. The COVID-19 pandemic has only worsened the situation, with people facing increased isolation, financial stress, and uncertainty about the future. The result is a behavioral health crisis that has swept the nation.
From urban centers to rural communities, the crisis has touched every corner of Rhode Island and the country, affecting individuals and families from all walks of life. BCBSRI is thankful for our behavioral health network providers and for their tireless work in helping those who are struggling with mental health and substance abuse disorders. Your dedication to your patients and your unwavering commitment to providing the best possible care, often in the face of difficult and complex cases, is inspiring. Your advocacy for better mental health policies and resources is helping to break down barriers to care and reduce the stigma surrounding mental illness.
Sadly, along with the rising demand for behavioral health services comes a growing trend of healthcare fraud. According to the National Health Care Anti-Fraud Association, mental health and substance abuse treatment fraud accounts for around $2 billion in losses each year. Some examples of this fraud include submitting false claims for services that were never provided, providing unnecessary or inappropriate treatments, and engaging in kickback schemes with other healthcare providers.
This type of fraud not only harms patients who may receive ineffective or harmful treatments, but it also drives up healthcare costs for everyone. It undermines the trust and integrity of the healthcare system and diverts resources away from those who truly need them. It’s important for healthcare providers, insurers, and regulatory agencies to remain vigilant and work in collaboration to prevent healthcare fraud in behavioral health. Only then can we ensure that patients receive the care they deserve and that are healthcare system operates fairly and efficiently. However, we realize that some of these claims issues may be due to a lack of education, so we wanted to provide a review of correct billing practices in behavioral health, some examples, and resources to learn more.
Coding for Evaluation and Management (E/M):
- In accordance with the 2021 American Medical Association (AMA) E/M coding changes for new and established E/M codes (99201-99215), psychiatric providers should perform a medically appropriate history and/or psychiatric examination with the goal of establishing medical necessity.
- The code selection no longer depends on the level of history or psychiatric exam.
- You should not consider comorbidities and underlying diseases when you select the E/M level unless they are addressed (evaluated or treated) during the visit.
- When performing an E/M alone, the level is based on medical decision making or time.
- To comply with the coding changes, documentation is very important to support the E/M level billed.
Coding for psychotherapy:
CPT describes psychotherapy as “the treatment of mental illness and behavioral disturbances in which the physician or other qualified healthcare professional, through definitive therapeutic communication, attempts to alleviate the emotional disturbances, reverse or change maladaptive patterns of behavior, and encourage personality growth and development."
Per CPT, psychotherapy codes are time-based:
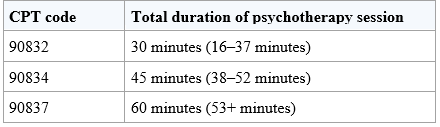
Example: Patient is seen for 40 minutes in the office for psychotherapy. Use code 90834 (45 minutes of psychotherapy).
For psychotherapy to be supported in the medical record, there must be documentation of therapeutic maneuvers, a periodic summary of goals, indication of progress, and/or documentation of a treatment plan. The time spent providing psychotherapy must be documented.
Coding for E/M with psychotherapy performed on the same day:
To bill an E/M and an add-on psychotherapy code, the two services must be significant and separately identifiable AND the time spent for each must be separate. The time used for medical management may not be included in the time of the psychotherapy. If less than 16 minutes are spent providing psychotherapy, the add-on psychotherapy cannot be billed. Additionally, the E/M level must be selected based on MDM and not time.
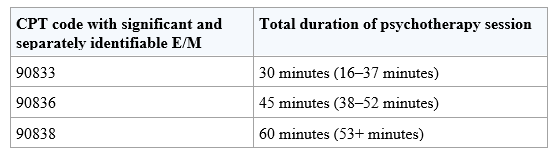
Example: Patient is seen in the office for an E/M visit with psychotherapy. The nature of the patient’s reason for visit and documentation meet criteria for a 99212 level E/M code. In addition to time spent on the E/M portion of the visit, 20 minutes are spent providing psychotherapy services. Both codes 99212 and 90833 (30 minutes psychotherapy add-on) are reported.
The documentation must support a separate and distinct description of the psychotherapy with patient-specific details. There must be documentation of therapeutic maneuvers, a periodic summary of goals, indicated progress, and/or documentation of a treatment plan.
Additional information and resources: